Aspirin for Primary Prevention of Cardiovascular Disease in Patients with Elevated Lp(a)
Discover the potential benefits of aspirin for individuals with elevated Lp(a) and learn how it can help reduce the risk of cardiovascular disease.
DR T S DIDWAL MD
9/2/20246 min read


According to an American College of Cardiology review, the growing evidence base suggests a potential benefit for aspirin use in primary prevention in individuals with elevated Lp(a), as demonstrated by secondary analyses of clinical trials using genetic instruments and observational studies using plasma Lp(a) levels. These studies highlight Lp(a)'s pro-thrombotic properties and the potential for aspirin to mitigate the associated cardiovascular risk. While the current class IIb recommendation in the 2019 ACC/AHA Guideline suggests considering aspirin in those 40 to 70 years of age with elevated ASCVD risk without increased bleeding risk, recent studies raise the possibility of a particular benefit in individuals with elevated Lp(a). Future randomized controlled trials are needed to better understand the risks and benefits associated with aspirin use in this population.
Key points
Elevated Lp(a) and Cardiovascular Risk: There's a need for strategies to offset the increased cardiovascular risk associated with high Lp(a) levels in primary prevention.
Aspirin and Lp(a): Secondary analyses of clinical trials and observational studies suggest that aspirin may reduce cardiovascular risk in individuals with elevated Lp(a).
Randomized controlled trials: Future randomized trials are necessary to better understand the risks and benefits of aspirin use in this population.
ACC/AHA Guideline: The current guideline recommends considering aspirin for primary prevention in those 40-70 years old with elevated ASCVD risk, but recent evidence suggests a potential benefit for individuals with elevated Lp(a).
Lp(a) and Aspirin: Lp(a)'s pro-thrombotic properties and aspirin's anti-platelet effects may explain the potential benefit of aspirin in those with elevated Lp(a).
Observational Studies: Recent observational studies have extended the findings from genetic instrument studies to plasma Lp(a) levels and broader populations.
Future Research: More randomized controlled trials are needed to confirm the benefits of aspirin in primary prevention for individuals with elevated Lp(a) and to better understand the balance of risks and benefits.
Potential of Aspirin for Elevated Lp(a)
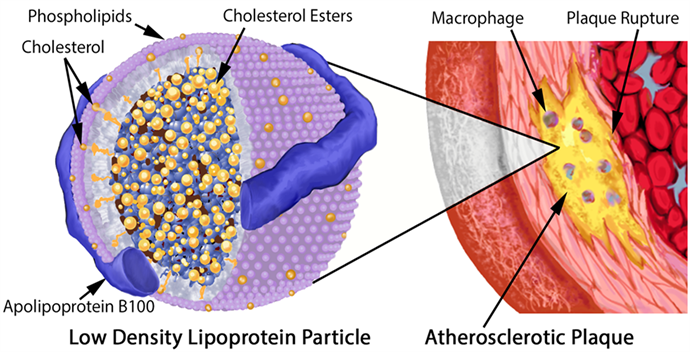
Lipoprotein(a) (Lp[a]) is a low-density lipoprotein (LDL) variant that carries a genetic predisposition to cardiovascular disease (CVD). Elevated Lp[a] levels are associated with an increased risk of atherosclerotic cardiovascular disease (ASCVD), including coronary artery disease, stroke, and peripheral artery disease. While statins can effectively lower LDL cholesterol, they have limited impact on Lp[a] levels. As a result, there is a pressing need for strategies to offset the increased cardiovascular risk associated with elevated Lp(a) in primary prevention.
Secondary Analyses and Observational Studies
Secondary analyses of clinical trials using genetic instruments and observational studies have shown promising results for aspirin in reducing cardiovascular risk in individuals with elevated Lp(a) in primary prevention settings. These studies have focused on carriers of specific single-nucleotide polymorphisms (SNPs) associated with increased Lp(a) levels and have observed a significant reduction in major adverse cardiovascular events (MACE) with aspirin use.
The Role of Lp(a) and Aspirin
Lp(a) is believed to contribute to cardiovascular risk through its pro-thrombotic properties, which may lead to increased platelet activation and aggregation. Aspirin, on the other hand, irreversibly inactivates cyclooxygenase 1 and limits thromboxane A2 production, reducing platelet activation. This interaction between Lp(a) and aspirin may explain the potential benefit of aspirin in individuals with elevated Lp(a).
ACC/AHA Guideline and Recent Updates
The American College of Cardiology/American Heart Association (ACC/AHA) Guideline on the Primary Prevention of Cardiovascular Disease has softened its prior recommendations regarding aspirin use for primary prevention, citing the small net cardiovascular benefit compared to the bleeding risk. However, recent studies have raised the possibility of a particular benefit for aspirin in individuals with elevated Lp(a).
Evidence for Aspirin in Primary Prevention with Elevated Lp(a)
Several studies have contributed to the growing evidence base supporting the potential benefit of aspirin in primary prevention for individuals with elevated Lp(a). Here are some of the key findings:
Genetic Instrument Studies: Secondary analyses of the Women's Health Study (WHS) and Aspirin in Reducing Events in the Elderly (ASPREE) trials found that aspirin use was associated with a significant reduction in MACE in carriers of specific SNPs associated with elevated Lp(a).
Observational Studies: The Multi-Ethnic Study of Atherosclerosis (MESA) and the National Health and Nutrition Examination Survey (NHANES III) have shown an association between aspirin use and a reduced risk of coronary heart disease (CHD) and ASCVD mortality in individuals with elevated Lp(a).
Limitations and Considerations
While the evidence is promising, it's important to consider the limitations of these studies. Genetic instrument studies are limited by the generalizability of their findings to the broader population, and observational studies are subject to confounding by indication and residual confounding. Additionally, the bleeding risk associated with aspirin use must be carefully weighed against the potential cardiovascular benefits.
Conclusion
The growing evidence base suggests that aspirin may be a promising strategy for reducing cardiovascular risk in individuals with elevated Lp(a). However, more research is needed to confirm its efficacy and safety in this population. Clinicians and patients need to weigh the potential benefits and risks of aspirin use on an individual basis.
Faqs:
1. Is elevated Lp(a) a risk factor for atherosclerosis?
Yes, elevated Lp(a) (lipoprotein(a)) is considered a risk factor for atherosclerosis. High levels of Lp(a) in the blood can contribute to the development of atherosclerotic plaques in arteries, increasing the risk of cardiovascular diseases such as heart attack and stroke.
2. What is a high Lp(a) level?
A high Lp(a) level is typically defined as above 30 mg/dL, although the exact threshold can vary depending on the laboratory and guidelines used. Some sources consider levels above 50 mg/dL as particularly high and associated with a greater risk of cardiovascular disease.
3. What causes high Lp(a) levels?
High Lp(a) levels are largely determined by genetics and can vary among individuals. Genetic mutations in the LPA gene lead to increased production of Lp(a) and higher blood levels. Other factors, such as hormonal changes or kidney disease, may also influence Lp(a) levels, but genetic factors are the primary cause.
4. What happens if Lp(a) levels are high?
If Lp(a) levels are high, it increases the risk of developing cardiovascular diseases such as atherosclerosis, heart attack, and stroke. Elevated Lp(a) can contribute to the buildup of plaques in the arteries and increase the likelihood of cardiovascular events. It's important for individuals with high Lp(a) levels to manage other risk factors and consult with a healthcare provider for appropriate monitoring and potential treatment strategies.
5. How is Lp(a) measured?
Lp(a) levels are measured through a blood test specifically designed to assess lipoprotein(a). This test is not typically included in standard cholesterol panels and may need to be requested separately by a healthcare provider.
6. Can lifestyle changes lower Lp(a) levels?
Lifestyle changes such as diet, exercise, and smoking cessation generally do not have a significant impact on Lp(a) levels, as these levels are primarily influenced by genetics. However, managing other cardiovascular risk factors through lifestyle changes is still important for overall heart health.
7. Are there any medications to lower Lp(a) levels?
Currently, there are limited options for directly lowering Lp(a) levels with medications. However, newer treatments, such as PCSK9 inhibitors and specific Lp(a)-lowering therapies, are being researched and may offer future solutions. In the meantime, managing other risk factors with medications like statins can help reduce cardiovascular risk.
8. How often should I have my Lp(a) levels checked?
The frequency of Lp(a) testing depends on individual risk factors and family history of cardiovascular disease. Generally, it is recommended to check Lp(a) levels if you have a personal or family history of heart disease, especially if you are at a young age or if cardiovascular disease occurs despite normal cholesterol levels.
9. Can high Lp(a) levels be treated or managed?
While direct treatment options for high Lp(a) are limited, managing other cardiovascular risk factors such as high LDL cholesterol, high blood pressure, and diabetes can help reduce overall cardiovascular risk. Emerging therapies and ongoing research may offer new treatment options in the future.
10. How does Lp(a) differ from LDL cholesterol?
Lp(a) and LDL cholesterol are both types of lipoproteins that can affect cardiovascular health, but they are distinct in their composition and impact. Lp(a) contains a unique protein called apolipoprotein(a), which is not present in LDL. While LDL cholesterol primarily contributes to plaque buildup in arteries, Lp(a) can also contribute to plaque formation and has additional implications for cardiovascular risk.
11. Is Lp(a) testing necessary for everyone?
Lp(a) testing is not routinely performed for everyone but may be recommended for individuals with a family history of cardiovascular disease, early onset of heart disease, or unexplained high cholesterol levels. Discussing with a healthcare provider can help determine if testing is appropriate for you based on your health profile and risk factors.
Journal Reference
What Should I Do About an Elevated Lp(a) Based on Current Evidence and Available Treatments? - American College of Cardiology. (2024, August 20). American College of Cardiology. https://www.acc.org/Latest-in-Cardiology/Articles/2024/08/20/12/59/accel-lite-20aug2024
Image credit: https://html.scirp.org/file/1-1910650x2.png
{kind=link}
Related
https://healthnewstrend.com/early-detection-of-heart-disease-in-women-3-key-biomarkers
Disclaimer
The information on this website is for informational purposes only and is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health care provider with any questions you may have regarding a medical condition or treatment. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.