Fatty Liver Disease & Obesity: Alarming Link & Essential Steps to Manage
Are you worried about fatty liver disease? Over 25% of adults have it, often linked to obesity. Learn about the risks, diagnosis, and lifestyle changes to slow its progression and protect your liver health.
DR T S DIDWAL MD
8/22/20248 min read


This document provides an overview of nonalcoholic fatty liver disease (NAFLD) and its potential progression to nonalcoholic steatohepatitis (NASH), focusing on their relevance to obesity management. Information is based on published research, the clinical perspectives of the Obesity Medicine Association (OMA), and peer review. Non-alcoholic fatty liver disease (NAFLD), affecting a staggering 25% of adults worldwide, is the most common chronic liver disease. Obesity is a major culprit, with over half of NAFLD patients having it. This raises the risk of developing the more severe NASH form, which is linked to increased heart disease risk, especially given its potential to progress to cirrhosis in 25% of cases within 9 years. While there's no cure, early detection and lifestyle changes like weight loss and healthy eating can slow its progression. Treatment might involve addressing underlying causes, medications like PPARg agonists, and even bariatric surgery in specific situations. Remember, factors beyond obesity, such as genetics and environment, can also play a role in NAFLD development. Early diagnosis and taking steps to manage weight and overall health are crucial for preventing its progression and potential complications.
Key Findings
NAFLD Prevalence and Association with Obesity:
NAFLD is the most common chronic liver disease, affecting over 25% of adults worldwide.
Obesity is a major risk factor for NAFLD, with over half to two-thirds of NAFLD patients having obesity.
Among those with NAFLD, 10–25% may progress to the more severe NASH form.
NAFLD and cardiovascular risk:
NAFLD is a risk factor for cardiovascular disease, with an even higher risk for NASH patients.
Obesity and type 2 diabetes further increase the risk of developing NASH.
NAFLD Definitions and Progression:
Hepatosteatosis, the initial stage of NAFLD, involves at least 5% liver fat accumulation.
NASH is defined by at least 5% liver fat with inflammation, cell injury, and potential fibrosis.
The risk of cirrhosis is low for fatty livers but increases significantly for NASH over time.
NAFLD Complications and Treatment:
NASH can lead to end-stage liver disease, and liver cancer, and require liver transplants.
While no approved drugs specifically treat NASH, lifestyle changes like weight loss and a healthy diet can slow the progression.
Imaging tests like transient elastography or MRI can help diagnose and assess NAFLD severity.
Treatment strategies include addressing underlying causes, promoting healthy lifestyle habits, and considering medications like PPARg agonists or GLP-1 receptor agonists in some cases.
Bariatric surgery may be an option for managing NAFLD in specific situations.
Additional Points:
Several factors beyond obesity can contribute to NAFLD, including genetics, medications, and environmental exposures.
The exact role of metformin in NAFLD treatment remains under investigation.
Hepatosteatosis, commonly known as fatty liver disease, is a prevalent condition characterized by the accumulation of fat in the liver cells. Diagnosis of hepatosteatosis is crucial for timely intervention and management. In this comprehensive guide, we delve into the various diagnostic methods available, including imaging tests and hepatic fibrosis tools.
Understanding Hepatosteatosis
Before diving into the diagnostic procedures, it's essential to grasp the basics of hepatosteatosis. This condition typically results in elevated liver transaminases such as alanine transaminase (ALT) and aspartate transaminase (AST), with normal bilirubin levels. An increase in ALT is often considered specific for non-alcoholic fatty liver disease (NAFLD). However, an AST: ALT ratio of >1.5 may indicate alcoholic liver disease, while AST > ALT is associated with increased hepatic fibrosis.
NAFLD Diagnosis: Imaging Tests
Liver Biopsy
Liver biopsy remains the definitive test for diagnosing NAFLD and its progressive form, non-alcoholic steatohepatitis (NASH). Despite its accuracy, liver biopsies are invasive and carry risks. They are currently required by the FDA for drug development programs targeting NAFLD/NASH.
Grading Hepatic Steatosis
Liver steatosis, or the accumulation of fat in hepatocytes, can be graded based on histological analysis:
Grade 0: <5%
Grade 1: 5–33%
Grade 2: 33–66%
Grade 3: >66%
Non-Invasive Hepatic Imaging
In clinical practice, non-invasive imaging techniques play a vital role in diagnosing NAFLD, especially in patients with risk factors such as obesity, hyperglycemia, and elevated ALT levels.
Liver Ultrasound
Liver ultrasound is widely available but may lack sensitivity, especially in detecting mild hepatic steatosis (<20% fat content). Despite this limitation, it remains a valuable initial screening tool.
Vibration-Controlled Transient Elastography (VCTE or Fibroscan®)
VCTE offers a non-invasive method to assess liver fat content (controlled attenuation parameter) and stiffness (fibrosis). While portable and radiation-free, its clinical availability may be limited due to cost constraints.
Computed Tomography (CT) and Magnetic Resonance Imaging (MRI)
CT is of limited use due to radiation exposure and accuracy issues in detecting mild steatosis. In contrast, MRI, particularly MRI-Proton Density Fat Fraction (MRI-PDFF), offers superior accuracy in assessing liver fat content without radiation exposure.
Magnetic Resonance Spectroscopy (MRS) and Elastography (MRE)
MRS measures fat content in small regions, while MRE accurately assesses liver fibrosis. Although highly accurate, MRE's availability may be limited compared to MRI-PDFF.
NAFLD Diagnosis: Hepatic Fibrosis Tools
Non-Invasive Fibrosis Assessment
Various tools are available for assessing hepatic fibrosis in adults, offering alternatives to liver biopsy:
NAFLD Activity Score
Fibrosis-4 Index (FIB-4)
NAFLD Fibrosis Score (NFS)
Enhanced Liver Fibrosis Score/Test
Fibrometer
FibroSure/FibroTest
Hepascore
These tools incorporate a combination of patient demographics and laboratory parameters to estimate fibrosis risk, providing valuable insights for clinical decision-making.
Liver biopsy stands as the gold standard for diagnosing non-alcoholic fatty liver disease (NAFLD) and its advanced form, non-alcoholic steatohepatitis (NASH). However, due to its invasive nature, alternative non-invasive imaging techniques are often preferred. Liver ultrasound, although readily available, may not be sensitive enough to detect mild cases of NAFLD. Vibration-controlled transient elastography (VCTE), commonly known as Fibroscan®, offers a non-invasive method to measure hepatic steatosis and fibrosis. Magnetic resonance imaging-proton density fat fraction (MRI-PDFF) provides a comprehensive assessment of liver fat content and is widely used in both clinical research and practice.
Causes and Risk Factors
Fatty liver disease can arise from a multitude of factors, including genetic predisposition, obesity, type 2 diabetes mellitus, insulin resistance, and metabolic syndrome. Excessive alcohol consumption remains a common cause of fatty liver disease. Additionally, certain medications and medical conditions, such as hepatitis C infection, polycystic ovarian syndrome, and cardiovascular disease, can contribute to the development of NAFLD.
Concomitant Medications and Uncommon Causes
Several medications have been associated with the development or exacerbation of NAFLD, including corticosteroids, amiodarone, and some antipsychotics. Furthermore, uncommon causes of NAFLD include autoimmune hepatitis, celiac disease, and mitochondrial defects in fatty acid oxidation.
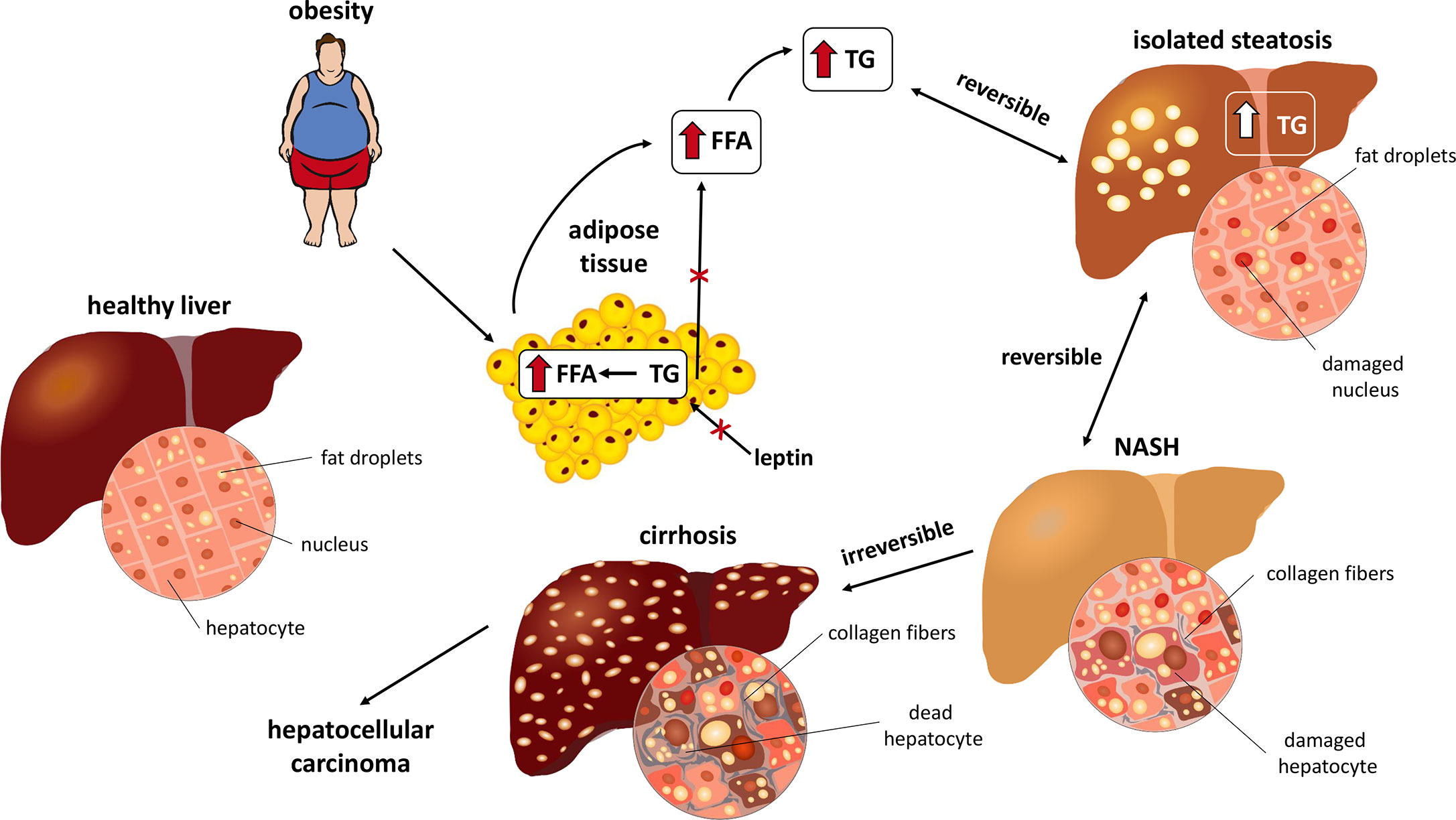
Mechanisms of NAFLD
The pathogenesis of NAFLD involves complex interactions between genetic, metabolic, and environmental factors. Adiposopathy, characterized by dysfunctional adipose tissue, plays a crucial role in the development of NAFLD. Increased circulating free fatty acids can lead to hepatic fat deposition, hepatocyte injury, inflammation, and fibrosis, ultimately resulting in fatty liver disease.
Metabolic Consequences of HFCS
The Composition of Fruits and Sugars
Fruits, characterized by their abundance of seeds and fiber, constitute a vital component of a balanced diet. The carbohydrate content of fruits typically consists of approximately 50% fructose and 50% glucose. While glucose is a simple sugar found in both animals and plants, fructose carries a lower glycemic index (GI) compared to glucose.
High Fructose Corn Syrup (HFCS) and Its Origins
High fructose corn syrup (HFCS), a widely used sweetener in processed foods and beverages, is derived from corn starch through enzymatic processes. This syrup, comprising approximately 50% fructose and 50% glucose, exhibits a glycemic index of around 70. Its sweetness surpasses that of sucrose, contributing to its widespread use as a sweetening agent.
Epidemiological Insights
Epidemiological data suggest a potential association between the consumption of sucrose, HFCS, and various metabolic disorders, including NAFLD, dyslipidemia, insulin resistance, and cardiovascular disease. The detrimental effects of these sugars on liver health extend beyond mere body weight gain or total energy intake. HFCS consumption has been linked to enhanced fatty acid synthesis, leading to increased hepatic diacylglycerols and interference with insulin signaling pathways. Moreover, fructose metabolism may stimulate hepatic gluconeogenesis, exacerbating metabolic imbalances associated with NAFLD.
Contrast with Natural Fruit Intake
In contrast to processed HFCS, the consumption of natural whole fruits offers distinct health benefits. Whole fruits, enriched with fiber and essential nutrients, are less likely to contribute to obesity and NAFLD. The presence of fiber in whole fruits mitigates the rapid absorption of sugars, offering a favorable impact on metabolic health.
Clinical Implications and Dietary Recommendations
Clinical evidence suggests that while HFCS consumption is strongly associated with NAFLD, the intake of unprocessed natural fruits is unlikely to contribute significantly to liver fat accumulation. Patients at risk of NAFLD are advised to limit their consumption of sugared drinks, fruit juices, red meat, processed meat, and saturated fats, opting instead for whole grains, lean meats, and plant-based protein sources.
Promoting Liver Health Through Dietary Choices
The path to liver health lies in adopting a balanced and nutrient-rich diet. Incorporating whole grains, lean proteins, and plant-based foods, such as fruits and vegetables, forms the cornerstone of dietary interventions aimed at preventing and managing NAFLD. Dietary patterns like the Mediterranean diet and Dietary Approaches to Stop Hypertension (DASH) have shown promising results in promoting liver health and overall well-being.
Nutritional Interventions for NAFLD
Medical Nutrition Therapy
Patients with NAFLD benefit from evidence-based meal plans designed to achieve a healthy body weight and optimize metabolic parameters. The Mediterranean diet, characterized by moderate consumption of lean proteins and restricted intake of saturated fats and refined carbohydrates, has emerged as a promising dietary approach for managing NAFLD.
Weight Loss Strategies
Weight loss remains a cornerstone of NAFLD management, with even modest reductions in body weight yielding significant improvements in hepatic steatosis and the histopathological features of non-alcoholic steatohepatitis (NASH). A weight loss of 3–5% is sufficient to ameliorate hepatic steatosis, while more substantial weight loss (7–10%) may be required to address NASH-related fibrosis.
Physical Activity and Exercise
Dynamic (Aerobic) and Resistance Training
Dynamic (aerobic) and resistance-based physical activity play pivotal roles in achieving and maintaining a healthy body weight, improving insulin sensitivity, and reducing circulating free fatty acids and glucose. Furthermore, physical activity promotes intrahepatic fatty acid oxidation, mitigates fatty acid synthesis, and prevents mitochondrial and hepatocellular damage, thereby exerting therapeutic effects on NAFLD independent of weight loss.
Benefits of Weight Reduction
Among individuals with pre-obesity or obesity, weight reduction of ≥10% through a combination of healthy nutrition and enhanced energy expenditure has demonstrated remarkable efficacy in improving NAFLD and NASH within a relatively short timeframe.
Pharmacotherapy for NAFLD
Current Pharmacological Options
While no pharmacotherapy has received regulatory approval specifically for NAFLD treatment, certain medications have shown promise in managing the condition and its complications.
Vitamin E: Supplementation with vitamin E (800 IU) may yield biochemical and histological improvements in liver fat among adult patients with NASH, although long-term use has been associated with an increased risk of prostate cancer.
Peroxisome Proliferator-Activated Receptor Gamma Agonists: Pioglitazone, a peroxisome proliferator-activated receptor gamma agonist, has demonstrated efficacy in reducing liver fat and improving NASH, despite potential increases in body weight.
Glucagon-Like Peptide-1 Receptor Agonists: Certain glucagon-like peptide-1 receptor agonists, such as liraglutide and semaglutide, have shown promise in reducing liver fat and improving NASH resolution, although further research is warranted.
Leptin Therapy: Leptin therapy may hold therapeutic potential for patients with lipodystrophy-associated NAFLD, although its efficacy requires further investigation.
Bariatric Surgery for NAFLD
Bariatric surgery, while primarily indicated for weight loss, has demonstrated ancillary benefits in improving liver histology, including fibrosis secondary to NASH. This underscores the interplay between obesity, metabolic health, and NAFLD pathogenesis, highlighting the potential role of surgical interventions in comprehensive disease management.
Conclusion
In conclusion, the treatment landscape for NAFLD is multifaceted, encompassing nutritional interventions, physical activity, medications, and, in select cases, surgical interventions. By adopting a holistic approach that addresses underlying metabolic imbalances and promotes lifestyle modifications, clinicians can effectively manage NAFLD and reduce the risk of associated complications. Continued research into novel therapeutic targets and personalized treatment strategies is essential to further optimize outcomes for patients with this prevalent liver condition.
Reference Article
Sara Karjoo, Anthony Auriemma, Teresa Fraker, Harold Edward Bays,Nonalcoholic fatty liver disease and obesity: An Obesity Medicine Association (OMA) Clinical Practice Statement (CPS) 2022, https://doi.org/10.1016/j.obpill.2022.100027.
Image credit:https://www.frontiersin.org/files/Articles/597583/fendo-11-597583-HTML/image_m/fendo-11-597583-g001.jpg
{kind=link}
Related
https://healthnewstrend.com/dementia-diagnosis-dont-miss-the-hidden-liver-connection
Disclaimer
The information on this website is for informational purposes only and is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health care provider with any questions you may have regarding a medical condition or treatment. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.