Type 1.5 Diabetes: Symptoms, Causes, Treatment of Latent Autoimmune Diabetes in Adults (LADA)
Discover the truth about LADA, often misdiagnosed as type 2 diabetes. Learn about the symptoms, causes, and treatment options for this autoimmune condition. Understand the differences between LADA and type 1 diabetes. Take control of your health with knowledge about LADA.
DR TS DIDWAL MD
8/15/202410 min read


Latent autoimmune diabetes in adults (LADA) is an often misunderstood type of diabetes that shares characteristics of both type 1 and type 2 diabetes. It's sometimes referred to as "type 1.5 diabetes." LADA is an autoimmune condition where the body's immune system attacks insulin-producing cells in the pancreas. Unlike type 1 diabetes, LADA progresses more slowly, often leading to misdiagnosis as type 2 diabetes. Key features of LADA include adult onset, presence of islet autoantibodies, initial insulin independence, and gradual decline in beta cell function. While LADA shares some risk factors with both type 1 and type 2 diabetes, its exact cause remains unclear. Managing LADA involves a combination of insulin therapy, oral medications, and lifestyle modifications. Early diagnosis and proper treatment are crucial for preserving beta cell function and preventing complications. Research into LADA is ongoing, with the aim of developing better diagnostic tools, treatments, and preventative strategies.
Key Points
1. LADA is a Misunderstood Diabetes Type
LADA shares characteristics of both type 1 and type 2 diabetes, but it's an autoimmune condition where the body attacks insulin-producing cells. Unlike type 1, LADA progresses more slowly, often leading to misdiagnosis as type 2.
2. LADA Onset and Symptoms
LADA typically develops in adulthood, often after age 30. Symptoms can be similar to type 2 diabetes, including increased thirst, frequent urination, and fatigue. However, LADA patients may not require insulin immediately.
3. Diagnosis and Testing
Diagnosing LADA can be challenging. It involves blood tests to check blood sugar levels and the presence of islet autoantibodies. These antibodies indicate an autoimmune attack on the pancreas.
4. LADA Progression
LADA is characterized by a gradual decline in beta cell function, which produces insulin. Over time, most LADA patients will require insulin therapy to manage their blood sugar levels.
5. LADA Management
Managing LADA focuses on maintaining blood sugar control. This involves a combination of insulin therapy, oral medications, and lifestyle changes, including diet, exercise, and weight management.
6. Importance of Early Diagnosis
Early diagnosis of LADA is crucial for effective management and preventing complications. Proper treatment can help slow the progression of the disease and improve overall health.
Latent Autoimmune Diabetes in Adults (LADA): An Often Misunderstood Form of Diabetes
Diabetes mellitus is a group of metabolic disorders characterized by high blood sugar levels over a prolonged period. While most people are familiar with type 1 and type 2 diabetes, there is another less well-known form called latent autoimmune diabetes in adults (LADA). LADA shares characteristics of both type 1 and type 2 diabetes, leading some to refer to it as "type 1.5 diabetes." LADA is an autoimmune form of diabetes that develops more slowly than classic type 1 diabetes. It is often misdiagnosed initially as type 2 diabetes due to its later onset in adulthood and the fact that patients may not require insulin immediately at diagnosis. However, LADA involves the autoimmune destruction of pancreatic beta cells, like type 1 diabetes.
In this comprehensive blog post, we will explore the characteristics, diagnosis, pathophysiology, and management of LADA in detail. Understanding this unique form of diabetes is crucial for proper diagnosis and treatment.
Prevalence and Epidemiology
LADA accounts for approximately 2–12% of all cases of diabetes in adults. Studies have found that 4–14% of patients initially diagnosed with type 2 diabetes actually have LADA when tested for islet autoantibodies. The prevalence appears to vary between different populations and countries, likely due to differences in diagnostic criteria, study designs, and lifestyle factors. In Western countries, the prevalence of LADA among patients diagnosed with type 2 diabetes ranges from about 3% to 10%. According to data from diabetes registries in Italy, the incidence of type 1 diabetes in adults aged 30-49 is similar to that in adolescents aged 15–19. Overall, LADA may be more common than previously thought, especially among adults diagnosed with diabetes between ages 30-50. Proper screening and diagnosis are important to identify these patients.
Clinical Characteristics and Presentation
LADA shares features of both type 1 and type 2 diabetes, which can make diagnosis challenging. Some key characteristics of LADA include:
Adult-onset, typically over age 30
Presence of islet autoantibodies (e.g. GAD antibodies)
Initial insulin independence for at least 6 months after diagnosis
Gradual decline in beta cell function over time
Lower BMI compared to typical type 2 diabetes
Less metabolic syndrome features than type 2 diabetes
Family history may or may not be present
Patients with LADA often present with symptoms similar to those of type 2 diabetes initially. They may have modest hyperglycemia that responds to oral medications at first. However, they tend to progress to insulin dependence faster than typical type 2 diabetes patients.
The rate of beta cell decline in LADA is generally slower than classic type 1 diabetes but faster than type 2 diabetes. This creates a window of opportunity for potential intervention to preserve beta cell function.
Pathophysiology and Immunology
The underlying cause of LADA is the autoimmune destruction of pancreatic beta cells, similar to type 1 diabetes. However, the autoimmune process tends to be slower and less aggressive compared to childhood-onset type 1 diabetes.
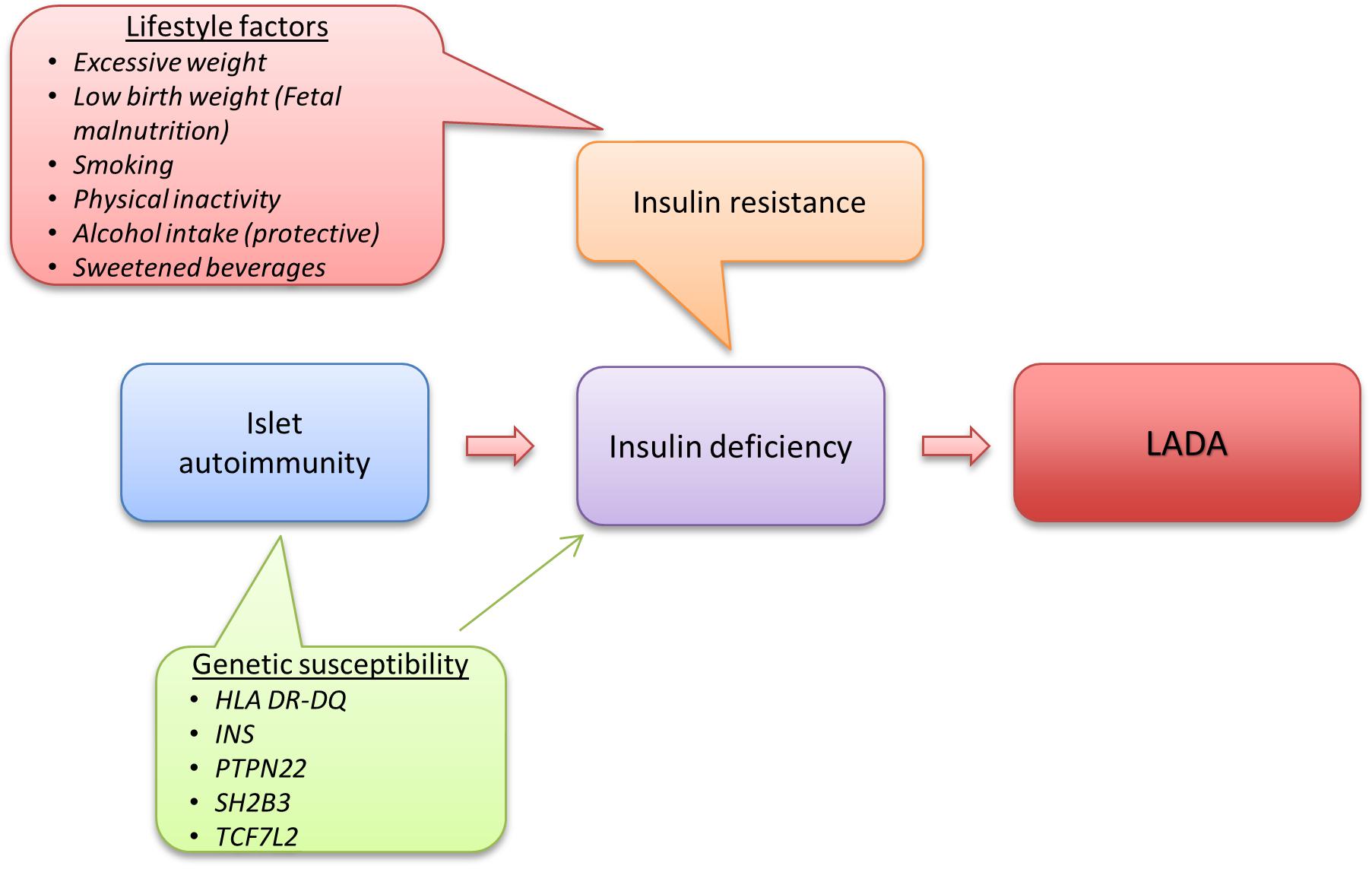
Key aspects of LADA pathophysiology include:
Autoantibodies: LADA patients have circulating autoantibodies against islet cell antigens, most commonly glutamic acid decarboxylase (GAD) antibodies. Other antibodies may include islet cell antibodies (ICA), insulin autoantibodies (IAA), and antibodies to tyrosine phosphatase-like protein IA-2.T cell-mediated autoimmunity: CD4+ and CD8+ T cells infiltrate the pancreatic islets and contribute to beta cell destruction. The T cell response may be less aggressive than in classic type 1 diabetes.
Genetic factors: LADA shares some genetic risk factors with both type 1 and type 2 diabetes. HLA genes confer the strongest genetic risk, similar to type 1 diabetes. Some type 2 diabetes-associated genes like TCF7L2 are also linked to LADA.
Innate immunity: Innate immune cells like macrophages and natural killer cells may play a role in the pathogenesis. Toll-like receptors (TLRs) on innate immune cells can trigger inflammatory responses.
Gut microbiome: Alterations in the intestinal microbiota may contribute to the autoimmune process in LADA. Studies have found differences in the gut microbiome of LADA patients compared to healthy controls and other types of diabetes.
Insulin resistance: Many LADA patients have some degree of insulin resistance, though typically less than in type 2 diabetes. This may contribute to the initial presentation resembling type 2 diabetes.
The interplay between adaptive immunity, innate immunity, and environmental factors leads to progressive loss of beta cell function in LADA, albeit at a slower rate than classic type 1 diabetes.
Diagnosis and Diagnostic Criteria
Diagnosing LADA can be challenging due to its overlapping features with both type 1 and type 2 diabetes. The Immunology and Diabetes Society has proposed the following criteria for LADA:
1. Adult age of onset (>30 years old)
2. Presence of any islet cell autoantibody
3. Absence of insulin requirement for at least 6 months after diagnosis
Testing for islet autoantibodies is crucial for identifying LADA. The most sensitive and specific test is for GAD autoantibodies. Other antibodies, like IA-2 and ZnT8, may also be present.
C-peptide levels can help assess residual beta cell function. LADA patients typically have detectable but declining C-peptide levels over time.
Some clinical features that may raise suspicion for LADA in a patient diagnosed with type 2 diabetes include:
Younger age at onset (30–50 years)
Lower BMI
Lack of metabolic syndrome features
Rapid progression to insulin requirement
personal or family history of other autoimmune diseases
proper diagnosis of LADA is important for appropriate treatment and monitoring. Misdiagnosis as type 2 diabetes may lead to delays in insulin therapy and faster loss of beta cell function.
Management and Treatment
The goals of LADA treatment are to achieve good glycemic control and preserve residual beta cell function as long as possible. Management should be individualized based on the patient's clinical presentation, rate of disease progression, and preferences.
Key aspects of LADA management include:
Insulin therapy: Most LADA patients will eventually require insulin. Early insulin treatment may help preserve beta cell function. Options include basal insulin, basal-bolus regimens, or insulin pump therapy.
Oral medications: Some oral agents may be used in early LADA, especially drugs that may have beta cell-protective effects. Options include:
DPP-4 inhibitors: May help preserve beta cell function and have anti-inflammatory effects
Metformin: Can help with insulin resistance?
Thiazolidinediones: May have immunomodulatory properties
GLP-1 receptor agonists: Can stimulate insulin secretion and may be beta cell protective
Sulfonylureas are generally avoided as they may accelerate beta cell failure.
Lifestyle modifications: A healthy diet, regular exercise, and weight management are important, similar to other forms of diabetes.
Autoantibody monitoring: Periodic testing of autoantibody levels may help guide treatment intensity.
Immunomodulatory therapies: Experimental treatments aimed at slowing the autoimmune process are an area of active research. Options being studied include:
GAD-alum vaccines
Anti-CD3 monoclonal antibodies
B cell depletion (e.g. rituximab)
Regulatory T cell therapy
Vitamin D supplementation
Management should be adjusted based on the individual patient's rate of beta cell decline and glycemic control. Close monitoring is important to determine when to intensify therapy.
Complications and Prognosis
The long-term complications of LADA are similar to other forms of diabetes and can include:
Microvascular complications: Retinopathy, nephropathy, and neuropathy
Macrovascular complications: Cardiovascular disease, stroke, peripheral artery disease
Hypoglycemia (especially with insulin therapy)
Diabetic ketoacidosis (rare)
Some studies have found that LADA patients may have a lower risk of complications compared to those with type 2 diabetes, possibly due to fewer metabolic syndrome features. However, other research has shown similar cardiovascular outcomes between LADA and type 2 diabetes. The prognosis of LADA depends on how quickly it is diagnosed and how well it is managed. With proper treatment, many patients can maintain good glycemic control and quality of life. However, most will progress to insulin dependence over time. Preserving beta cell function for as long as possible is a key goal. This may help reduce the risk of complications and maintain better glycemic control. Early diagnosis and appropriate management are crucial for optimizing outcomes in LADA.
Future Directions and Research
LADA is an active area of research, with many unanswered questions about its pathophysiology, natural history, and optimal management. Some key areas of ongoing investigation include:
Biomarkers: Identifying better biomarkers to distinguish LADA from type 2 diabetes and predict disease progression.
Immunotherapies: Developing targeted immunomodulatory treatments to preserve beta cell function.
Gut microbiome: Understanding the role of the intestinal microbiota in LADA pathogenesis and potential therapeutic targets.
Genetic factors: Further elucidating the genetic basis of LADA and how it differs from type 1 and type 2 diabetes.
Personalized medicine: Developing tools to predict individual disease course and response to different therapies.
Prevention strategies: Exploring ways to prevent or delay onset in high-risk individuals.
Novel insulin formulations: Creating better insulin preparations for physiologic replacement.
Artificial pancreas technology: Advancing closed-loop insulin delivery systems for LADA management.
As our understanding of LADA grows, management strategies will likely become more tailored and effective. The ultimate goal is to prevent beta cell loss and maintain normal glucose homeostasis without the need for exogenous insulin.
Conclusion
Latent autoimmune diabetes in adults represents a unique form of diabetes with features of both type 1 and type 2 diabetes. Its gradual onset and initial insulin independence can lead to misdiagnosis as type 2 diabetes. However, the presence of islet autoantibodies and progressive beta cell loss distinguish LADA as an autoimmune form of diabetes. Proper diagnosis of LADA is crucial for appropriate management. Treatment should aim to preserve beta cell function while maintaining good glycemic control. A combination of insulin therapy, oral medications, lifestyle modifications, and potentially immunomodulatory treatments may be used. As research in this field progresses, our understanding of LADA pathophysiology and management continues to evolve. Future advances in biomarkers, immunotherapies, and personalized medicine hold promise for improving outcomes in LADA patients. Healthcare providers should maintain a high index of suspicion for LADA, especially in younger adults diagnosed with type 2 diabetes who do not fit the typical phenotype. With increased awareness and proper management, patients with LADA can achieve good glycemic control and reduce their risk of complications.
Faqs
What is the difference between LADA and type 1 diabetes?
While both LADA and type 1 diabetes are autoimmune conditions that affect the pancreas, LADA develops more slowly and often in adults, while type 1 typically appears in childhood. LADA patients may produce some insulin initially, whereas type 1 patients usually require insulin immediately.
What are the symptoms of LADA?
Symptoms of LADA are similar to type 2 diabetes and include increased thirst, frequent urination, fatigue, blurred vision, and slow-healing wounds. However, LADA patients may also experience weight loss, unlike those with type 2 diabetes.
How is LADA diagnosed?
LADA is diagnosed through blood tests to check blood sugar levels and the presence of islet autoantibodies. These antibodies indicate an autoimmune attack on the pancreas. A C-peptide test may also be used to assess insulin production.
What is the treatment for LADA?
LADA treatment focuses on managing blood sugar levels. It typically involves a combination of insulin therapy, oral medications, and lifestyle changes such as diet, exercise, and weight management.
Can LADA be cured?
Currently, there is no cure for LADA. However, with proper management, people with LADA can live healthy and fulfilling lives.
What is the life expectancy of someone with LADA?
With good blood sugar control and management of related health conditions, people with LADA can have a normal life expectancy. However, it's essential to follow recommended treatment plans and monitor for complications.
Is LADA hereditary?
While having a family history of autoimmune diseases can increase the risk of developing LADA, it's not directly inherited. Genetic factors play a role, but environmental factors also contribute to the development of LADA.
Can you prevent LADA?
There's no known way to prevent LADA, as its exact causes are still being studied. Maintaining a healthy lifestyle, including a balanced diet, regular exercise, and weight management, can help support overall health but may not prevent LADA.
What are the complications of LADA?
Like other types of diabetes, LADA can lead to complications if not managed well. These complications include heart disease, stroke, kidney disease, nerve damage, eye problems, and foot problems.
How common is LADA?
LADA is less common than type 1 and type 2 diabetes, but its prevalence is increasing. It's estimated to account for 5-10% of adult-onset diabetes cases.
References
1.Ravikumar, V., Ahmed, A., & Anjankar, A. (2023). A Review on Latent Autoimmune Diabetes in Adults. Cureus, 15(10), e47915. https://doi.org/10.7759/cureus.47915
2.Hu, J., Zhang, R., Zou, H., Xie, L., Zhou, Z., & Xiao, Y. (2022). Latent Autoimmune Diabetes in Adults (LADA): From Immunopathogenesis to Immunotherapy. Frontiers in endocrinology, 13, 917169. https://doi.org/10.3389/fendo.2022.917169
Image credit:https://www.frontiersin.org/files/Articles/438244/fphys-10-00320-HTML/image_m/fphys-10-00320-g005.jpg
{kind=link}
Related
https://healthnewstrend.com/how-do-carbohydrates-affect-blood-sugar-control-in-diabetics
Disclaimer
The information on this website is for informational purposes only and is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health care provider with any questions you may have regarding a medical condition or treatment. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.