Muscle Loss & Fat Gain: Unraveling Sarcopenic Obesity in Older Adults
Struggling with muscle loss and weight gain as you age? You might have sarcopenic obesity. Learn about this condition, its causes, diagnosis, and effective management strategies like exercise, diet, and potential treatments. Improve your health and maintain mobility!
DR T S DIDWAL MD
8/12/20245 min read


Sarcopenic obesity, characterized by concurrent declines in muscle mass and function alongside increases in adipose tissue, presents a significant public health concern for older adults. This review, published in Nature Reviews Endocrinology, examines the multifaceted pathophysiology, diagnostic challenges, and current and emerging management strategies for this condition. This complex condition arises from hormonal shifts, chronic inflammation, and lifestyle choices like inactivity and poor diet. Diagnosing it accurately involves muscle mass assessment, functional tests, and inflammation markers. Fortunately, management strategies exist, including exercise, protein-rich diets, and potential medications.
Key Points:
Definition: Sarcopenic obesity is a condition characterized by both muscle loss (sarcopenia) and excess body fat.
Risk Factors: Aging, poor diet, lack of physical activity, and certain medical conditions contribute to sarcopenic obesity.
Health Consequences: This condition increases the risk of falls, fractures, heart disease, diabetes, and overall mortality.
Diagnosis: Assessing muscle mass, strength, and function, along with body fat percentage, is crucial for diagnosing sarcopenic obesity.
Treatment: A combination of exercise, especially resistance training, a balanced diet rich in protein, and sometimes medication can help manage sarcopenic obesity.
Prevention: Regular physical activity, a healthy diet, and weight management are essential for preventing sarcopenic obesity.
Importance of Early Detection: Early diagnosis and intervention can help slow the progression of sarcopenic obesity and improve quality of life.
Introduction:
Sarcopenic obesity (SO), characterized by both muscle loss (sarcopenia) and excess fat mass, poses a significant health threat, especially for older adults. While ageing typically leads to muscle loss alongside fat gain, this condition can also occur at any age due to obesity's negative impact on muscle health. Several factors contribute to this vicious cycle, including chronic diseases, a sedentary lifestyle, inappropriate diets, and even weight loss efforts. Importantly, SO amplifies the risks associated with both obesity and sarcopenia, impacting mobility, increasing dependence, and leading to disability. It even contributes to bone structure changes and osteoporosis. Beyond affecting quality of life, SO is strongly linked to frailty, various chronic diseases, and increased mortality, making it a major public health concern.
Pathophysiology:
The intricate interplay of various factors contributes to sarcopenic obesity, including:
Hormonal Shifts: Age-related decline in anabolic hormones like estrogen and testosterone, coupled with elevated cortisol, promotes muscle catabolism and weakens anabolic processes.
Chronic Inflammation: Persistent low-grade inflammation disrupts muscle protein synthesis and repair, further exacerbating muscle loss.
Muscle and Adipose Tissue Changes: Dysregulation of adipocyte function and altered skeletal muscle fibre composition contribute to impaired muscle function and fat accumulation.
Lifestyle Factors: Physical inactivity and poor nutrition negatively impact muscle mass and function, while excess energy intake promotes adiposity.
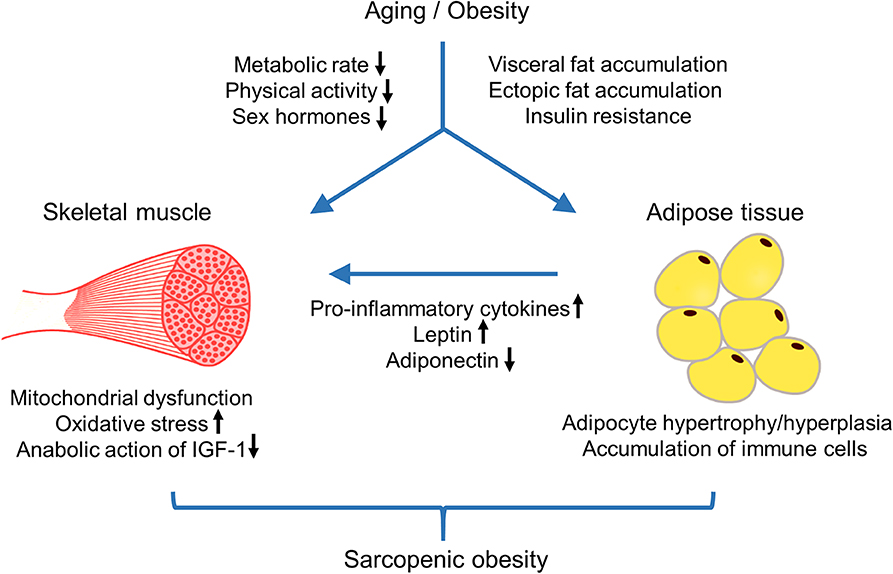
1. Endocrine Crosstalk:
Adipose tissue, our fat storage hub, sends mixed signals. Pro-inflammatory cytokines like IL-6 and TNF-α from excess fat damage muscle.
Leptin, meant to promote muscle growth, seems blunted in sarcopenic obesity, suggesting resistance to its action.
Adiponectin, which regulates muscle metabolism, shows elevated levels but reduced effectiveness, possibly fueling protein breakdown.
2. Muscle Determinants:
Protein balance is disrupted, with muscle breakdown exceeding synthesis.
Specific muscle fiber types crucial for force generation, and daily activities shrink.
Stem cell function in muscles declines, potentially due to impaired mitochondrial dynamics and energy burden.
Increased fat within muscle cells (IMCL) contributes to insulin resistance and anabolic resistance, further hindering muscle growth.
3. Mitochondrial Dysfunction:
High-fat diets and aging worsen mitochondrial function, limiting muscle's ability to burn fat for energy.
Key enzymes for fatty acid oxidation are compromised, leading to IMCL accumulation.
Targeting mitochondria to enhance fatty acid oxidation may be a promising therapeutic approach.
Diagnosis:
While officially a disease, diagnosing sarcopenic obesity, the combination of muscle loss and excess fat, remains challenging due to:
Lack of universal criteria: BMI for obesity and gait speed/lean mass for muscle loss offer starting points, but specifics evolve.
Stage-based approach: screening involves BMI/waist circumference and muscle loss hints, followed by muscle function tests and body composition analysis.
There is no official disease code: Diagnosis involves fitting the evolving definition and managing risks based on symptoms and age.
Muscle Mass Assessment: Techniques like DXA quantify muscle mass and distribution.
Functional Testing: Gait speed, grip strength, and other assessments evaluate functional limitations.
Biomarkers: C-reactive protein and other markers may indicate the presence of inflammatory processes.
Management Strategies:
While a definitive cure remains elusive, a multi-pronged approach is crucial:
Lifestyle Interventions: Regular physical activity, particularly strength training, is paramount. A balanced diet rich in protein, essential micronutrients, and adequate calorie intake supports muscle anabolism.
Nutritional Considerations: Protein supplementation and dietary interventions tailored to address individual needs play a vital role in optimizing muscle health.
Pharmacological Therapies: In specific cases, testosterone therapy or other medications may be considered to address hormonal imbalances or inflammation.
Emerging Therapies: Personalized medicine approaches and gene therapy hold promise for targeted interventions in the future.of
Exercise:
Resistance training: This is the cornerstone, promoting muscle strength and function in a dose-dependent manner. Programs can be tailored to individual needs and abilities, with benefits seen in both men and women.
Aerobic exercise: While not as potent as resistance training for muscle mass, it helps reduce body fat and improve overall fitness, contributing to better function and quality of life.
Combination training: This approach, combining resistance and aerobic exercises, offers the best of both worlds, improving muscle performance and reducing fat mass effectively.
Diet:
Adequate protein intake: Ensuring enough protein, ideally 0.8–1 gram per kilogram of body weight, is crucial for preventing muscle loss and potentially improving function.
Dietary modification: While calorie restriction is standard for obesity, it can harm muscle. Tailored dietary approaches may help control weight without sacrificing muscle, often emphasizing fruits, vegetables, and whole grains.
Supplementation: Micronutrients like vitamin D, selenium, and magnesium, along with protein supplements like whey, can address deficiencies and support muscle function, but personalized consultation is recommended.
Medical interventions:
Hormone therapy: Testosterone replacement in men and estrogen in postmenopausal women may be options to restore hormonal balance and improve muscle mass and function, but careful evaluation and monitoring are crucial due to potential risks.
Whole-body electromyostimulation (WB-EMS): This technique uses electrical pulses to stimulate muscle contractions, improving body composition and function, but its effectiveness varies and may not be suitable for everyone.
Oxytocin therapy: This emerging approach uses intranasal oxytocin to improve lean mass in older adults, but its impact on muscle function remains unclear and requires further research.
Key considerations:
Tailored approach: Every individual is unique, requiring personalized treatment plans considering age, health conditions, and preferences.
Combining strategies: Often, the best results come from combining different interventions like exercise, diet, and potentially specific supplements or therapies, guided by healthcare professionals.
Safety and monitoring: Regular monitoring and close consultation with healthcare providers are essential throughout the treatment process to ensure safety and effectiveness.
Collaboration and Technology:
Combating sarcopenic obesity necessitates collaboration between:
Clinicians: Early diagnosis, personalized treatment plans, and ongoing monitoring are crucial for effective management.
Researchers: Continued research into the complex interplay of factors and the development of novel interventions is essential.
Individuals: Active participation in lifestyle modifications and adherence to treatment plans empower individuals to manage their condition.
Digital technologies like telehealth, wearable devices, and educational apps can enhance accessibility, provide real-time data, and offer support for self-management.
Conclusion:
Sarcopenic obesity presents a complex challenge, but a comprehensive understanding of its pathophysiology and the implementation of evidence-based management strategies, combined with collaborative efforts and technological advancements, offer hope for improved health outcomes and quality of life for older adults.
Reference Article
Prado, C.M., Batsis, J.A., Donini, L.M. et al. Sarcopenic obesity in older adults: a clinical overview. Nat Rev Endocrinol (2024). https://doi.org/10.1038/s41574-023-00943-z
Image credit:https://www.frontiersin.org/files/Articles/530178/fendo-11-00332-HTML/image_m/fendo-11-00332-g001.jpg
{kind=link}
https://healthnewstrend.com/obesity-and-heart-health-unveiling-the-complex-connection
Medical Disclaimer
The information on this website is for informational purposes only and is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health care provider with any questions you may have regarding a medical condition or treatment. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.