The Role of Obesity Medications in Maintaining Muscle During Weight Loss
"Discover how obesity medications can not only help you lose weight but also preserve or even increase muscle mass. Learn about the latest research on GLP-1 receptor agonists, tirzepatide, and other promising drugs. Explore the importance of resistance training and protein intake for optimizing body composition during weight loss."
DR T S DIDWAL MD
9/24/202411 min read
According to a review article in the International Journal of Obesity Obesity medications have shown significant weight loss effects and potential benefits beyond mere reduction in body weight. One area of particular interest is the impact of these drugs on body composition, especially muscle mass. Preserving or even increasing muscle mass during weight loss is crucial for metabolic health, glucose regulation, functional capacity, weight loss maintenance, and overall health. Recent obesity medications, such as GLP-1 receptor agonists (liraglutide, semaglutide) and the dual GIP/GLP-1 receptor agonist tirzepatide, have shown promising results in terms of body composition, potentially preserving or even increasing muscle mass. However, more research is needed to fully understand the long-term effects of these medications on body composition and to develop strategies for maximizing muscle preservation during weight loss. Combining these medications with resistance training and ensuring adequate protein intake may be beneficial.
Key points
Muscle mass is crucial for obesity treatment. It contributes to metabolic health, glucose regulation, functional capacity, weight loss maintenance, and overall health.
Obesity medications can have positive effects on body composition. Some drugs, such as GLP-1 receptor agonists and tirzepatide, may help preserve or even increase muscle mass.
Liraglutide has shown promising results in preserving muscle mass. Studies have found that liraglutide treatment leads to significant reductions in fat mass while maintaining lean body mass.
Semaglutide may also preserve muscle mass. While some lean mass loss is observed, the preservation of a higher proportion of lean mass relative to fat mass is encouraging.
Tirzepatide has shown significant improvements in body composition. It may lead to reductions in both fat mass and lean mass, but the ratio of fat mass to lean mass loss is favorable.
Naltrexone/bupropion can help preserve muscle mass. This combination medication has shown positive effects on body composition, with minimal muscle loss.
Resistance training and adequate protein intake are important. These factors can help maximize the muscle-preserving effects of obesity medications.
Obesity Pharmacotherapy: Beyond Weight Loss: Exploring Effects on Muscle Mass
Obesity is a complex chronic disease that affects millions of people worldwide. It's associated with numerous health complications, including type 2 diabetes, cardiovascular disease, and certain types of cancer. While lifestyle interventions like diet and exercise remain the cornerstone of obesity treatment, pharmacotherapy has emerged as a promising adjunctive approach. Recent advancements in obesity medications have not only shown significant weight loss effects but also potential benefits beyond mere reduction in body weight. One area of particular interest is the impact of these drugs on body composition, especially muscle mass.
The Importance of Muscle Mass in Obesity Treatment
Before delving into the specifics of obesity pharmacotherapy, it's crucial to understand why maintaining or even increasing muscle mass during weight loss is so important:
Metabolic health: Muscle tissue is metabolically active, contributing significantly to overall energy expenditure. More muscle mass means a higher basal metabolic rate, which can help with long-term weight management.
Glucose regulation: muscles play a vital role in glucose uptake and metabolism, helping to maintain healthy blood sugar levels.
Functional capacity: Adequate muscle mass is essential for mobility, balance, and overall physical function, especially as we age.
Weight loss maintenance: Preserving muscle mass during weight loss can help prevent the metabolic slowdown often associated with dieting, making it easier to maintain weight loss in the long term.
Overall health: Muscle mass is associated with better overall health outcomes, including improved cardiovascular health and reduced risk of chronic diseases.
Given these benefits, an ideal obesity treatment would not only reduce fat mass but also preserve or even increase muscle mass. This is where obesity pharmacotherapy comes into play.
Overview of Current Obesity Medications
Several medications have been approved for the treatment of obesity in recent years. Let's look at some of the most promising ones:
GLP-1 Receptor Agonists
Liraglutide (Saxenda®): Originally developed for type 2 diabetes treatment, liraglutide at higher doses was approved for obesity treatment in 2014.
Semaglutide (Wegovy®): A more potent GLP-1 receptor agonist, semaglutide, was approved for obesity treatment in 2021.
Dual GIP/GLP-1 Receptor Agonist
Tirzepatide: While primarily developed for type 2 diabetes (approved as Mounjaro®), tirzepatide has shown remarkable weight loss effects and is being studied for obesity treatment.
Combination Therapy
Naltrexone/Bupropion (Contrave®): This combination medication works on the central nervous system to reduce appetite and food cravings.
These medications have demonstrated significant weight loss effects in clinical trials, often surpassing the efficacy of older obesity drugs. But what about their effects on muscle mass?
Effects of Obesity Medications on Muscle Mass
Emerging evidence suggests that some obesity medications may have positive effects on body composition, potentially preserving or even increasing muscle mass during weight loss. Let's explore the current understanding of each drug's impact:
Liraglutide (Saxenda®)
Liraglutide, a GLP-1 receptor agonist, has shown promising results in terms of body composition. A study published in the journal "Diabetes, Obesity and Metabolism" in 2019 found that liraglutide treatment led to significant reductions in fat mass while preserving lean body mass in overweight and obese adults with type 2 diabetes.
The study, which lasted 26 weeks, compared liraglutide to placebo and found that:
Liraglutide-treated patients lost an average of 4.3 kg of body weight.
74% of the weight loss was from fat mass.
Lean body mass was preserved in the liraglutide group, while it decreased slightly in the placebo group.
These findings suggest that liraglutide may offer a favorable body composition profile during weight loss, potentially helping to maintain muscle mass.
Semaglutide (Wegovy®)
Semaglutide, a more potent GLP-1 receptor agonist, has shown even more dramatic weight loss effects than liraglutide. While most studies have focused on total weight loss, some have also examined body composition changes.
A sub-study of the STEP 1 trial, presented at the European Congress on Obesity in 2021, investigated the effects of semaglutide on body composition:
Participants lost an average of 15.3 kg with semaglutide vs. 2.6 kg with placebo over 68 weeks.
About 70% of the weight loss with semaglutide was fat mass.
Lean body mass also decreased, but proportionally less than fat mass, resulting in an overall improvement in body composition.
While this study shows some loss of lean mass, the preservation of a higher proportion of lean mass relative to fat mass is encouraging. However, more research is needed to fully understand semaglutide's effects on muscle mass, particularly when combined with resistance exercise.
Tirzepatide
Tirzepatide, a dual GIP/GLP-1 receptor agonist, has shown remarkable weight loss effects in clinical trials for type 2 diabetes. While not yet approved for obesity treatment, its potential in this area is significant.
A study published in "The Lancet" in 2021 examined the effects of tirzepatide on body composition in patients with type 2 diabetes:
Participants lost up to 11.9 kg of body weight over 40 weeks.
Significant reductions were seen in both fat mass and lean mass.
The ratio of fat mass to lean mass loss was favorable, indicating an improvement in overall body composition.
These results suggest that tirzepatide may lead to significant improvements in body composition. However, as with semaglutide, strategies to specifically preserve muscle mass (such as resistance training) may be beneficial in conjunction with the medication.
Naltrexone/Bupropion (Contrave®)
The combination of naltrexone and bupropion works differently from the GLP-1 based therapies, primarily affecting appetite and food cravings through central nervous system mechanisms.
A study published in "Obesity" examined the effects of naltrexone/bupropion on body composition:
Participants lost an average of 5.4 kg of body weight over 56 weeks.
The majority of weight loss (85%) was from fat mass.
Lean body mass was largely preserved, with only a small decrease noted.
These findings suggest that naltrexone/bupropion may help preserve lean mass during weight loss, although the total weight loss is generally less than that seen with GLP-1 based therapies.
Mechanisms of Action and Muscle Mass
Understanding how these medications might influence muscle mass requires a closer look at their mechanisms of action:
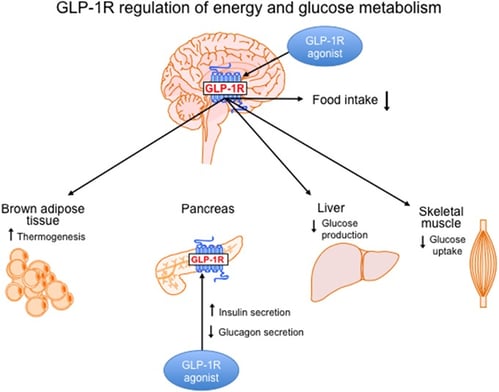
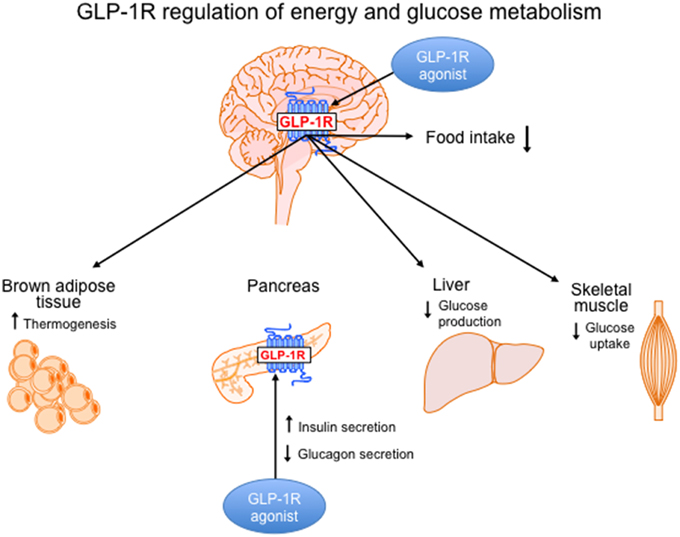
GLP-1 Receptor Agonists (Liraglutide, Semaglutide):
The primary action is on appetite regulation through central nervous system effects.
May improve insulin sensitivity, which could indirectly benefit muscle metabolism.
Some evidence suggests direct effects on muscle tissue, potentially improving glucose uptake and protein synthesis.
Dual GIP/GLP-1 Receptor Agonist (Tirzepatide):
Combines the effects of GLP-1 with those of glucose-dependent insulinotropic polypeptide (GIP).
May have more potent effects on glucose metabolism and potentially on muscle tissue.
The exact mechanisms of its effects on body composition are still being studied.
Naltrexone/Bupropion:
Works primarily through appetite regulation and possibly by modulating reward pathways.
Less direct effect on muscle tissue, but by promoting weight loss without excessive muscle catabolism, it may indirectly help preserve muscle mass.
It's important to note that while these mechanisms suggest potential benefits for muscle mass, the primary effect of all these medications is weight loss. The challenge lies in maximizing fat loss while minimizing muscle loss.
Potential Downsides of Obesity Medications:
While obesity medications have shown promising results, they are not without potential risks:
Gastrointestinal side effects: Nausea, vomiting, diarrhea, and constipation are common side effects.
Pancreatitis: In rare cases, GLP-1 receptor agonists can cause pancreatitis.
Hypoglycemia: For people with diabetes, these medications can increase the risk of hypoglycemia.
Thyroid tumors: GLP-1 receptor agonists have been linked to an increased risk of thyroid tumors, though the risk is low.
Muscle mass loss: Some medications, while preserving muscle mass compared to fat loss, may still lead to some lean mass loss.
Medications Still Under Development:
Several new obesity medications are in development, with the potential to offer different benefits and side effects:
Bimagrumab: This medication is being studied in combination with semaglutide to potentially preserve muscle mass during weight loss.
Other GLP-1 receptor agonists: Several new GLP-1 receptor agonists are being investigated, with the goal of improving efficacy and reducing side effects.
Novel mechanisms of action: Researchers are exploring medications that target different biological pathways involved in obesity, such as the endocannabinoid system and the central nervous system.
It's important to note that the risks and benefits of obesity medications can vary depending on the individual and the specific medication. Consult with a healthcare professional for personalized advice.
Considerations for Clinical Practice
Given the potential effects of obesity medications on muscle mass, clinicians should consider several factors when developing treatment plans:
Comprehensive approach: Pharmacotherapy should be part of a comprehensive obesity treatment plan that includes dietary intervention, physical activity, and behavioral modifications.
Resistance training: Encouraging patients to engage in resistance exercise may help maximize the muscle-preserving effects of these medications.
Protein intake: Ensuring adequate protein intake is crucial for muscle preservation during weight loss. This may be especially important for patients on GLP-1 based therapies, which can reduce overall food intake.
Monitoring body composition: When possible, using methods to assess body composition (such as DEXA scans or bioelectrical impedance) can provide more insight than scale weight alone.
Individualized treatment: The choice of medication should be based on individual patient factors, including their starting body composition, overall health status, and weight loss goals.
Long-term perspective: Consider the long-term effects on body composition and metabolic health, not just short-term weight loss.
Future Directions and Research Needs
While the current evidence on obesity medications and muscle mass is promising, several areas require further research:
Long-term studies: Most current data comes from relatively short-term studies. Longer-term research is needed to understand the effects of these medications on body composition over time.
Combination with exercise: Studies examining the combined effects of these medications with structured exercise programs, particularly resistance training, could provide valuable insights.
Mechanisms of action: More research is needed to fully understand how these medications affect muscle tissue at a cellular and molecular level.
Comparative studies: Head-to-head comparisons of different obesity medications in terms of their effects on body composition would be valuable for clinical decision-making.
Special populations: Studies focusing on specific populations (e.g., the elderly, those with sarcopenic obesity) could help tailor treatments more effectively.
Conclusion
Obesity pharmacotherapy represents a significant advance in the treatment of obesity, offering benefits that go beyond simple weight loss. The potential effects of these medications on body composition, particularly in preserving or even increasing muscle mass, add another dimension to their therapeutic value.
As our understanding of these medications grows, we may be able to develop more targeted approaches to obesity treatment that not only reduce excess fat but also optimize overall body composition. This could lead to improved metabolic health, better functional outcomes, and more sustainable long-term weight management.
However, it's crucial to remember that these medications are not magic bullets. They work best as part of a comprehensive approach to obesity treatment that includes dietary changes, increased physical activity, and behavioral modifications. The potential muscle-preserving effects of these drugs should be seen as a valuable tool in this broader treatment strategy.
For clinicians, staying informed about the latest research in this rapidly evolving field is crucial. As we gain more insights into how these medications affect body composition, we'll be better equipped to tailor treatments to individual patient needs, potentially leading to better outcomes in obesity management.
For individuals struggling with obesity, these advancements offer new hope. The possibility of losing weight while maintaining muscle mass could make the weight loss journey more effective and sustainable. However, it's important to approach these treatments under the guidance of a healthcare professional who can provide personalized advice and monitoring.
As research continues to unfold, the future of obesity treatment looks promising. By focusing not just on weight loss, but on optimizing body composition, we may be able to achieve better health outcomes and improve quality of life for millions of people affected by obesity.
Faqs
Can weight loss medications be used if you have obesity?
Yes, weight loss medications, also known as obesity pharmacotherapy, can be used as part of a comprehensive treatment plan for obesity. These medications can help you lose weight and improve your overall health. However, they should not be used as a substitute for healthy lifestyle changes, such as diet and exercise.
Can obesity pharmacotherapy help you lose weight?
Yes, obesity pharmacotherapy can help you lose weight. Several medications have been approved for the treatment of obesity, and they can help you lose a significant amount of weight. However, it's important to remember that these medications work best when combined with healthy lifestyle changes.
What is obesity pharmacotherapy?
Obesity pharmacotherapy is the use of medications to treat obesity. It can be a helpful tool for people who are struggling to lose weight with diet and exercise alone. However, it's important to talk to your doctor to see if obesity pharmacotherapy is right for you.
How do obesity medications work?
Obesity medications work in different ways. Some help to reduce appetite, while others help to block the absorption of fat. All obesity medications work best when combined with healthy lifestyle changes.
Are there any side effects to obesity medications?
Yes, there are some side effects to obesity medications. Common side effects include:
Nausea
Diarrhea
Constipation
Headache
Dizziness
Fatigue
How long do I need to take obesity medications?
You may need to take obesity medications for several months or even years. However, your doctor will monitor your progress and adjust your medication as needed.
Can I stop taking obesity medications after I lose weight?
It's important to talk to your doctor before stopping taking obesity medications. In some cases, you may need to continue taking them to maintain your weight loss.
Are obesity medications safe?
Obesity medications are generally safe when taken as prescribed. However, it's important to talk to your doctor about any potential risks before starting treatment.
Can I take obesity medications if I have other health conditions?
If you have other health conditions, it's important to talk to your doctor before taking obesity medications. Some medications may not be safe for people with certain health conditions.
Can I take obesity medications if I'm pregnant or breastfeeding?
If you're pregnant or breastfeeding, you should not take obesity medications.
Can I take obesity medications if I'm taking other medications?
If you're taking other medications, it's important to talk to your doctor before taking obesity medications. Some medications may interact with each other.
How much do obesity medications cost?
The cost of obesity medications varies depending on the type of medication and your insurance coverage.
Can I get obesity medications over the counter?
No, obesity medications are only available by prescription.Sources and related content
Related Articles:
1.The Complex Web of Obesity-Associated Comorbidities: A Comprehensive Overview
2.Fat Loss: More Than Just Burning Calories
Journal Reference
Argyrakopoulou, G., Gitsi, E., Konstantinidou, S. K., & Kokkinos, A. (2024). The effect of obesity pharmacotherapy on body composition, including muscle mass. International Journal of Obesity, 1-7. https://doi.org/10.1038/s41366-024-01533-3
Hope, D. C., & Tan, T. M. (2024). Skeletal muscle loss and sarcopenia in obesity pharmacotherapy. Nature Reviews Endocrinology, 1-2. https://doi.org/10.1038/s41574-024-01041-4
Shi, Q., Wang, Y., Hao, Q., Vandvik, P. O., Guyatt, G., Li, J., Chen, Z., Xu, S., Shen, Y., Ge, L., Sun, F., Li, L., Yu, J., Nong, K., Zou, X., Zhu, S., Wang, C., Zhang, S., Qiao, Z., . . . Li, S. (2024). Pharmacotherapy for adults with overweight and obesity: A systematic review and network meta-analysis of randomised controlled trials. The Lancet, 403(10434), e21-e31. https://doi.org/10.1016/S0140-6736(24)00351-9
Image credit: :https://www.frontiersin.org/files/Articles/137519/fnins-09-00092-HTML/image_m/fnins-09-00092-g001.jpg
{kind=link}
Disclaimer